


Breastfeeding Initiation: A Professional Guide to Establishing Milk Supply
The first hours and days after birth are a critical window for establishing breastfeeding. Understanding the physiological process of lactogenesis (milk production) and practical techniques for successful initiation can help new mothers navigate this important period. This guide provides evidence-based information on how to start breastfeeding and what to expect during the first feeds.
*Disclaimer: This information is for educational purposes only and does not replace professional medical advice. Always consult your midwife, lactation consultant, or healthcare provider for concerns about breastfeeding.*
1. Understanding the Stages of Milk Production
Before discussing techniques, it’s helpful to understand the physiological stages your body goes through:
| Stage | Timing | What Happens |
|---|---|---|
| Lactogenesis I | Mid-pregnancy onwards | Body produces colostrum (first milk) |
| Lactogenesis II | Day 2-5 postpartum | Copious milk “comes in”—triggered by delivery of placenta (drop in progesterone) |
| Lactogenesis III | Established breastfeeding | Milk supply shifts to autocrine control (supply = demand) |
Key point: Your body has been preparing for breastfeeding since mid-pregnancy. The first feeds are about colostrum—small volumes but rich in antibodies and nutrients. Progesterone withdrawal after birth provides the trigger for lactogenesis in the presence of high prolactin levels .
2. How to Initiate Breastfeeding After Birth
The First Hour After Birth
WHO and UNICEF recommend initiating breastfeeding within the first hour of birth . This window is critical for both mother and baby.
Immediate steps:
1. Skin-to-skin contact immediately after birth
– Place baby naked (with a warm blanket over both of you) on your chest
– Continue uninterrupted for at least the first hour or until after the first feed
– Benefits: stabilises baby’s temperature, heart rate, and blood sugar; triggers instinctive feeding behaviours
2. Allow baby to self-attach
– Most healthy newborns placed skin-to-skin will instinctively crawl toward the breast and self-attach
– This process may take 20-60 minutes—be patient
– Avoid rushing or forcing the baby onto the breast
3. Offer the breast
– If baby shows feeding cues (rooting, sucking movements, hand-to-mouth), gently guide them to the breast
– Aim for the first feed within the first hour
What if baby doesn’t feed immediately?
– Continue skin-to-skin—it’s still beneficial
– Hand express colostrum and offer on a spoon or with a syringe
– Seek help from midwife or lactation consultant
Important research note: A 2023 study found that delaying breastfeeding initiation to >1 to ≤24 hours after birth is **not associated with decreased breastfeeding duration** compared with initiating at ≤1 hour, for both vaginal and cesarean deliveries . While early initiation remains recommended, this may reassure mothers who experience delays.
First 24-48 Hours: Colostrum Phase
During this period, your breasts produce colostrum—thick, yellowish, nutrient-dense first milk.
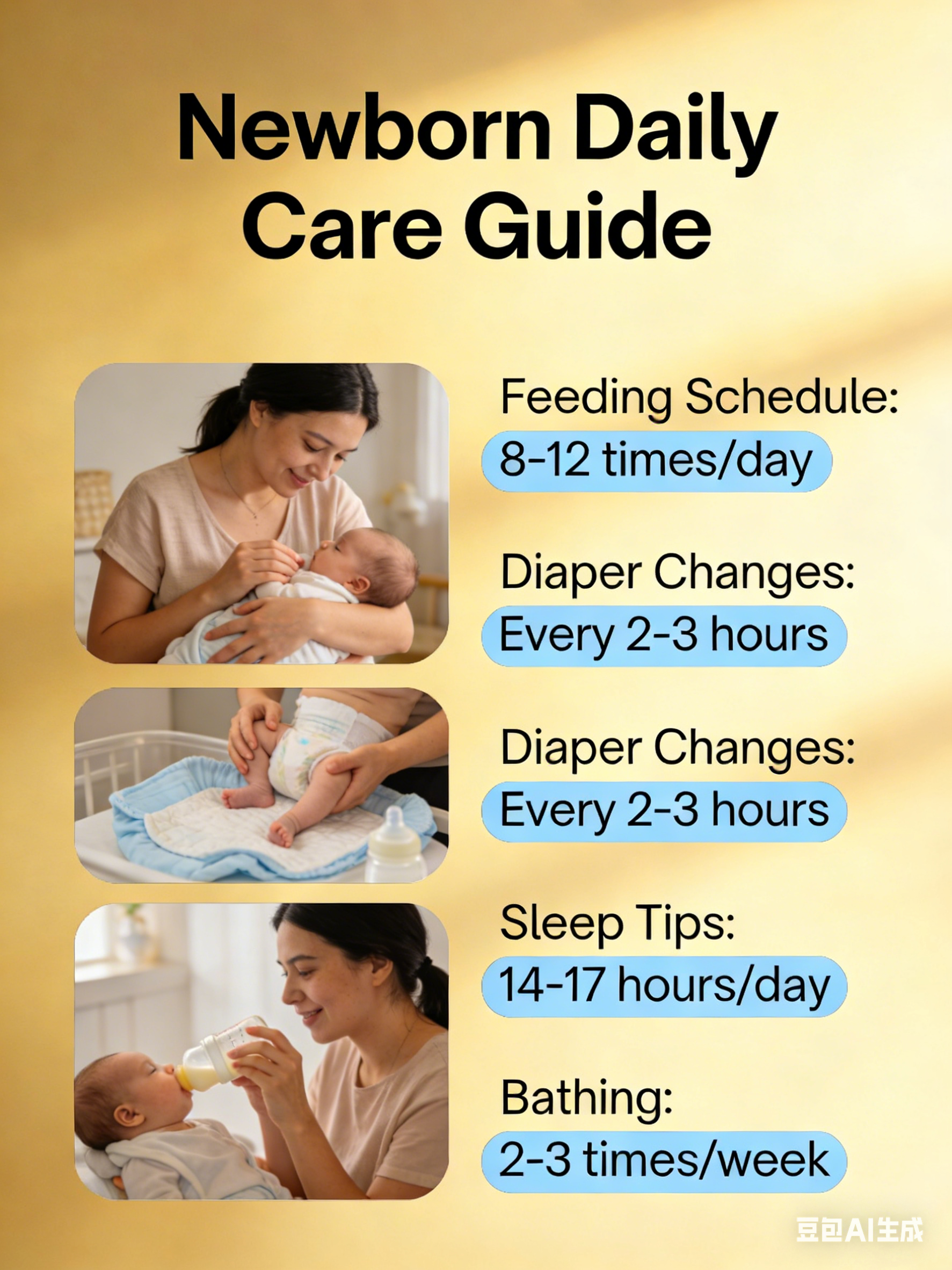
Feeding frequency:
– Newborns need 8-12 feeds in 24 hours
– Feeds may be frequent and irregular
– Follow baby’s cues, not the clock
What to expect:
– Small volumes (baby’s stomach is the size of a cherry at birth)
– Colostrum is concentrated—small amounts meet baby’s needs
– Wet nappies: Day 1: 1-2, Day 2: 2-3, Day 3: 3-4 (increasing as milk comes in)
Physiology note: Failure of early removal of colostrum from the breast is associated with high milk sodium and poor prognosis for successful lactation . Frequent feeding helps establish supply.
Day 3-5: Milk “Coming In”
As milk volume increases, breasts may feel full, firm, and warm—this is called engorgement and is most common 3-5 days after birth .
Continue:
– Frequent feeding (8-12 times/24 hours)
– Responsive feeding—watch baby, not the clock
– Skin-to-skin contact to stimulate milk production
3.First Feed: What to Expect and What to Do
Before the Feed
Position yourself comfortably:
– Sit or lie down in a relaxed position
– Use pillows to support your back and arms
– Bring baby to breast, not breast to baby
– Ensure you’re relaxed—tension can inhibit let-down
Try different positions:
– Laid-back position (biological nurturing): Lean back in a chair or bed, baby lies on top of you tummy-to-tummy. This triggers newborn reflexes and helps baby self-attach .
– Cross-cradle hold: Sit upright, support baby’s back and neck with opposite hand to the breast being used. Good for newborns learning to latch .
– Side-lying hold: Lie on your side with baby facing you. Useful for rest and cesarean recovery .
During the Feed
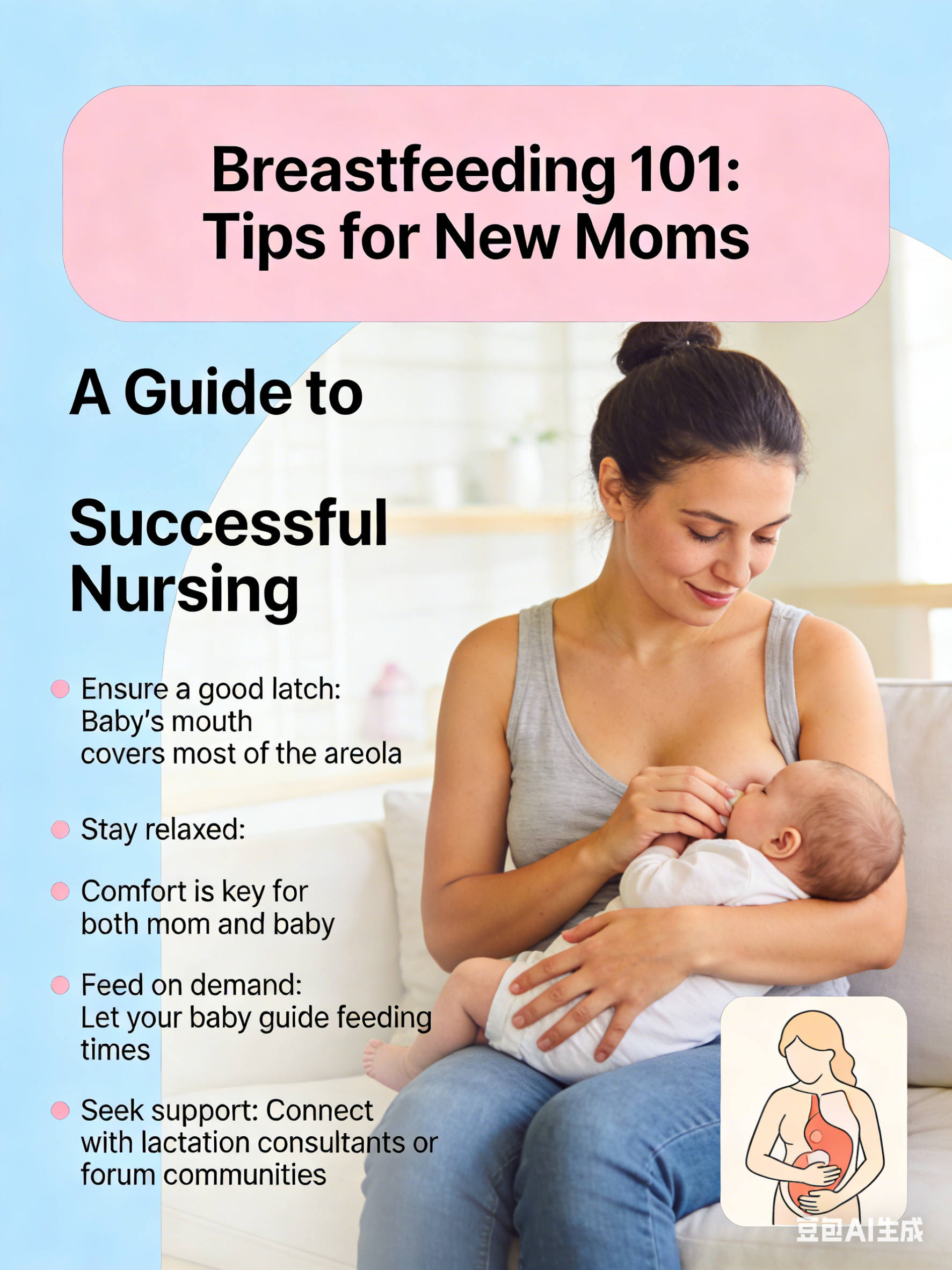
Achieving a good latch (the “asymmetric” latch):
The key to effective, pain-free breastfeeding is a deep, asymmetric latch where baby takes more of the areola with the lower jaw than the upper.
| Sign of Good Latch | Sign of Poor Latch |
|---|---|
| Baby’s mouth wide open (like a yawn) | Mouth not opened wide |
| Lower lip turned out | Lips tucked in |
| Chin touching breast | Chin away from breast |
| More areola visible above top lip than below | Even amount of areola visible |
| No pain (beyond initial mild tugging) | Pinching or pain throughout feed |
| Rhythmic sucking with audible swallowing | Shallow, rapid sucking |
| Baby settled and content after feed | Baby fussy, still hungry after feed |
How to achieve a good latch:
1. Support breast with hand (C-hold: thumb on top, fingers below, well back from areola)
2. Tickle baby’s lips with nipple to encourage wide opening
3. When mouth opens wide like a yawn, bring baby quickly onto breast—**baby goes to breast, breast does not go to baby**
4. Aim nipple toward baby’s palate (roof of mouth)
For flat or inverted nipples:
– Roll the nipple between your fingers before feeding
– Hand express or briefly pump before latching to draw out nipple
– Babies “breastfeed,” not “nipple feed”—their suck can draw the nipple in
Signs baby is feeding effectively:
– Jaw movement right back to the ear
– Swallowing sounds (soft “kah” sound)
– Feels like gentle tugging, not pinching
– Breasts feel softer after feed
After the Feed
– Allow baby to finish naturally (may come off spontaneously)
– If you need to break suction, insert clean finger into corner of baby’s mouth
– Express a drop of milk and rub onto nipple—helps healing
– Change feeding positions for next feed to drain all breast areas
4. First-Time Feeding: Key Points to Remember
It’s a Learning Process for Both of You
– Breastfeeding is a learned skill for both mother and baby
– It’s normal for early feeds to feel awkward or take practice
– Most challenges resolve with time and support
Pain Is Not Normal
– Mild tugging sensation at latch-on is normal during the first week
– Initial soreness should wear off 15-30 seconds after baby latches
– Persistent pinching, cracking, or bleeding nipples indicate a problem
– If soreness continues beyond the first week or worsens, seek help
Baby’s Output Matters More Than Input
– Wet nappies and stool frequency are better indicators than perceived milk intake
– Day 1-2: 1-3 wet nappies, meconium stools (black, tarry)
– Day 3-4: 4-6 wet nappies, transitional stools (greenish-brown)
– Day 5+: 6+ heavy wet nappies, yellow seedy stools (breastfed)
Responsive Feeding Is Key
– Feed when baby shows early hunger cues (rooting, sucking fists, lip smacking)
– Crying is a late hunger cue—try to feed before baby reaches this stage
– Avoid scheduled feeding—follow baby’s lead
Avoid Supplements Unless Medically Indicated
– Avoid water, formula, or glucose water unless prescribed
– These interfere with milk supply and may increase allergy risk
– If supplementation is medically necessary (e.g., low blood sugar, dehydration), expressed breast milk is first choice
Use Both Breasts
– Offer first breast until baby comes off or slows sucking
– Offer second breast (baby may or may not take it)
– Alternate which breast you start with at each feed
Manage Engorgement
If breasts become hard, sore, and too full when milk comes in:
– Hand express a little milk before feeding to soften areola
– Apply something cool to breasts after feeds to reduce swelling
– Feed frequently—empty breasts signal continued production
Look After Yourself
– Keep water within reach during feeds
– Eat regular, nutritious meals
– Rest when possible—tiredness affects milk production
– Limit caffeine and avoid alcohol
– Accept help from others
5. Common First-Time Challenges and Solutions
| Challenge | What to Do |
|---|---|
| Baby seems sleepy, not interested in feeding | Undress baby (keep warm blanket over back), gentle stimulation (tickle feet, stroke cheek), skin-to-skin contact |
| Nipples sore or cracked | Check latch; express a little milk and rub onto nipples after feeds; use pure lanolin if recommended; seek lactation support |
| Engorgement (breasts hard, full) | Feed frequently; hand express a little before feed to soften areola; cold packs after feeds |
| Baby not latching | Skin-to-skin; try different positions (laid-back position especially helpful) ; hand express colostrum onto nipple to encourage; seek help |
| Worried baby isn’t getting enough | Monitor wet nappies (see above); attend baby’s weight checks; trust your body—most mothers produce enough |
| Flat or inverted nipples | Roll nipples between fingers; hand express or pump briefly before latching; breastfeed still possible |
| Blocked duct or mastitis symptoms | Continue breastfeeding from affected side; empty breast often; rest; apply cold packs; seek medical help if fever or worsening |
6. When to Seek Help
Contact your midwife, health visitor, or lactation consultant if:
– Baby has fewer than expected wet nappies
– Baby is unusually sleepy and difficult to wake for feeds
– Baby has jaundice (yellow skin/eyes) that worsens
– You experience severe pain throughout feeds
– Breasts become red, hot, or you develop fever (possible mastitis)
– You’re worried about your baby’s feeding or weight gain
– You’re feeling overwhelmed or struggling emotionally
Most breastfeeding difficulties are resolvable with prompt, skilled support.
7. Summary: First Week Breastfeeding Checklist
| Day | Focus |
|---|---|
| Day 1 (birth) | Skin-to-skin, first feed within hour, colostrum |
| Day 2 | Frequent feeds (8-12x), monitor wet nappies (2-3), continue skin-to-skin |
| Day 3-5 | Milk coming in—breasts fuller, feed responsively, wet nappies increasing (4-6), manage engorgement if needed |
| Day 6-7 | Check weight (may have regained birth weight by day 10-14), continue as above |
Key resources:
– Association of Breastfeeding Mothers: www.abm.me.uk
– La Leche League: www.laleche.org.uk
– National Breastfeeding Helpline: 0300 100 0212
*References available upon request. Key sources: WHO/UNICEF Baby Friendly Initiative , NHS Start for Life, PubMed studies , New Zealand Ministry of Health , Norwegian Directorate of Health .*
a.本站所有文章,如无特殊说明或标注,均为本站原创发布。
b.任何个人或组织,在未征得本站同意时,禁止复制、盗用、采集、发布本站内容到任何网站、书籍等各类媒体平台。
c.如若本站内容侵犯了原著者的合法权益,可联系我们进行处理。









暂无评论内容