

Feeding and Weaning: A Professional Guide to Infant Cues, Common Challenges, and Transitioning from Breastfeeding
Understanding your baby’s feeding cues, managing common issues like choking and nursing strikes, and navigating the weaning process are essential skills for every breastfeeding parent. This guide provides evidence-based information to help you recognize hunger and satiety signals, handle feeding difficulties safely, and transition your baby from breast to other foods smoothly.
*Disclaimer: This information is for educational purposes only and does not replace professional medical advice. Always consult your health visitor, GP, or lactation consultant for concerns about your baby.*
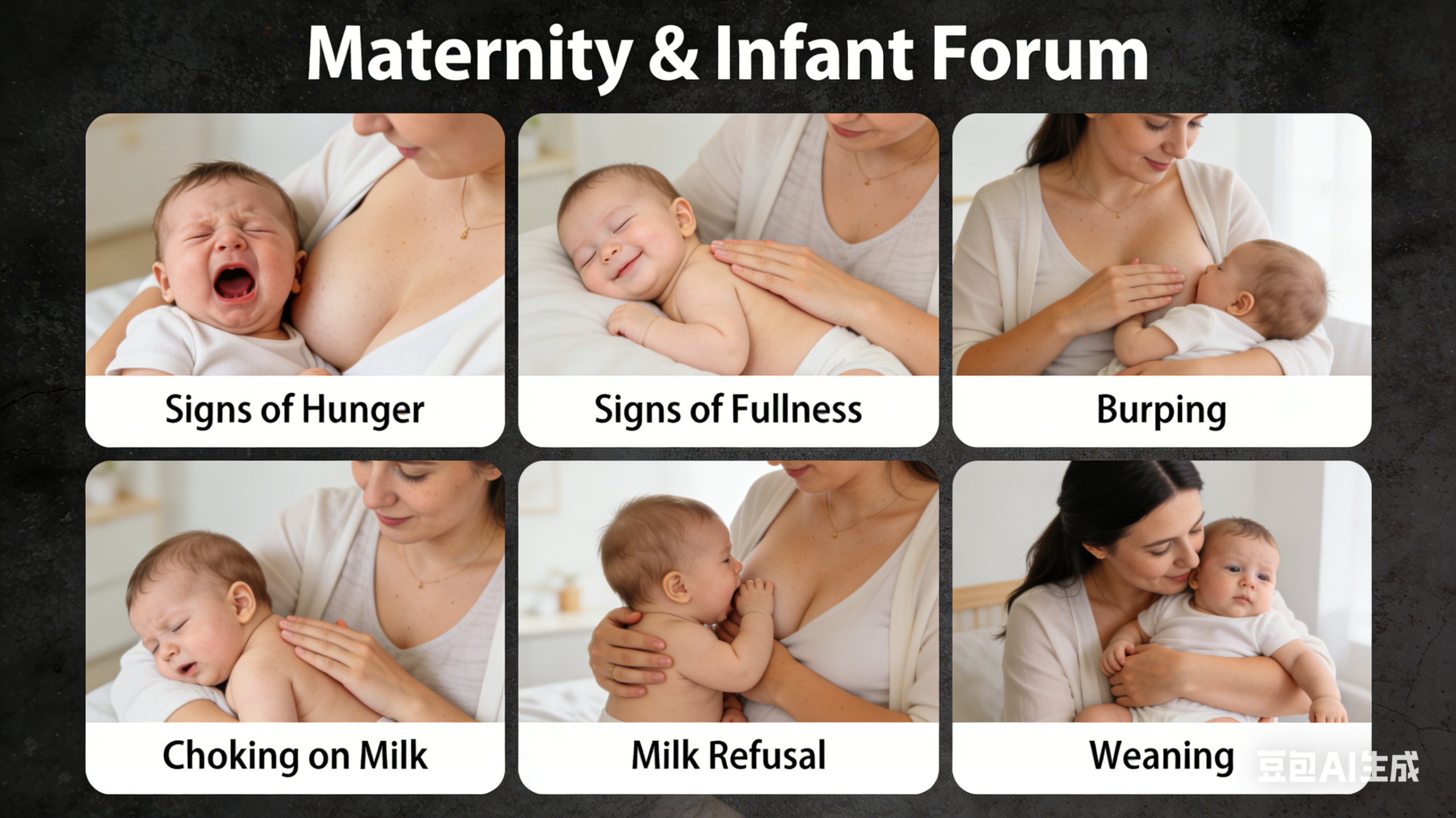
Part 1: Recognizing Hunger and Fullness Cues
How to Tell If Your Breastfed Baby Is Hungry
Babies communicate their need to feed through a series of progressive cues. Responding to early cues makes feeding easier and baby more settled .
Early hunger cues (best time to feed):
– Rooting (turning head and opening mouth when cheek is stroked)
– Sucking on fists or fingers
– Lip smacking or licking lips
– Becoming more alert or active
– Squirming or fidgeting
Mid hunger cues (still can feed but may be harder to latch):
– Stretching
– Increased physical movement
– Hand-to-mouth movements
Late hunger cues (fussy baby, may need calming before feeding):
– Crying (a late sign of hunger)
– Agitation
– Turning red
Key point: Crying is a late hunger cue. Try to feed before your baby reaches this stage, as a crying baby may have difficulty latching properly .
How to Tell If Your Breastfed Baby Is Full
Recognizing when your baby has had enough is equally important. Responsive feeding means allowing the baby to guide the feeding session.
Signs baby is full:
– Releasing or pushing away from the breast
– Slowing down or stopping sucking
– Unlatching spontaneously
– Falling asleep and releasing the breast
– Appearing relaxed and content
– Hands are open (not clenched) and body relaxed
– Turning head away from breast when offered again
Caregivers should take active care in feeding by being responsive to the child’s clues for hunger and also encouraging the child to eat . This principle applies to breastfeeding and, later, to complementary feeding.
Part 2: Burping Your Baby
Why Burping Matters
When babies feed, they may swallow air along with milk. This trapped air can cause discomfort, gas, and spitting up. Burping helps release this air.
How to Correctly Burp Your Baby
Three effective positions can help release trapped air:
| Position | How to Do It | Tips |
|---|---|---|
| Over the shoulder | Hold baby upright with chin resting on your shoulder. Support head and back with one hand. Gently pat or rub baby’s back with the other hand. | Use a burp cloth to protect your clothing. |
| Sitting on lap | Sit baby on your lap facing away from you. Support baby’s chest and head with one hand. Gently pat or rub back with the other hand. | Lean baby slightly forward to create gentle pressure on tummy. |
| Lying across lap | Lay baby face-down across your lap, supporting head (which should be slightly higher than chest). Gently pat or rub back. | Good for babies who don’t burp easily in other positions. |
Technique tips:
– Use gentle, rhythmic patting or circular rubbing motions
– Burp in the middle of a feed (when switching breasts) and at the end
– Not all babies need to burp after every feed—follow your baby’s cues
– If no burp after a few minutes but baby seems comfortable, it’s fine to stop
Important: After feeding, place baby on their back for sleep. Always supervise your baby and avoid propping bottles or leaving baby unattended during feeding .
Part 3: Managing Choking (Choking on Milk)
Choking occurs when milk enters the airway instead of the esophagus. Understanding how to respond can be life-saving.
Why Babies Choke
Newborns and infants have immature neurological systems, which can affect the function of the epiglottis—the “flap” that directs food to the esophagus and air to the windpipe. When this mechanism fails, milk can enter the airway, causing choking .
Risk Factors for Choking
– Feeding when baby is overly hungry (feeds too eagerly)
– Incorrect feeding position
– Oversupply or forceful let-down
– Prematurity or certain medical conditions affecting sucking/swallowing
Prevention Strategies
– Feed before baby becomes overly hungry
– Keep baby in a semi-upright position during feeding
– Choose appropriate bottle nipple flow rate (for formula-fed babies)
– Pause if milk flows too quickly or if baby seems overwhelmed
– After feeding, hold baby upright and burp before laying down
How to Respond If Baby Chokes
Mild choking (baby can cough, cry, or breathe):
– Stay calm and let baby cough—coughing is the most effective way to clear the airway
– Turn baby to the side to help milk drain
– Gently pat baby’s back with the heel of your hand, supporting head and neck
– Use gauze or a cloth to gently wipe away milk from mouth and nose
Severe choking (baby cannot breathe or make sounds, turns blue):
This is a medical emergency requiring immediate action. According to the American Heart Association’s 2025 guidelines, the sequence for infant choking rescue is **5 back blows followed by 5 chest thrusts** .
Infant choking rescue (under 1 year) – AHA 2025 guidelines :
Step 1: 5 Back Blows
– Position baby face-down along your forearm, holding the jaw (not the throat) with your hand
– Keep baby’s head lower than their body (about 30° angle)
– Using the heel of your free hand, deliver **5 firm back blows** between the shoulder blades
Step 2: 5 Chest Thrusts
– Turn baby over, supporting the back of the head with your hand
– Place baby face-up on your thigh, head still lower than body
– Using **one hand’s palm**, deliver **5 quick chest thrusts** in the center of the chest, just below the nipple line (depth about 4 cm, or 1/3 of chest depth)
– Allow chest to fully rise between thrusts
Step 3: Repeat
– Continue cycles of 5 back blows and 5 chest thrusts until the object is expelled or baby becomes unresponsive
If baby becomes unresponsive:
– Immediately begin CPR (30 chest compressions followed by 2 rescue breaths)
– Call emergency services (999 in UK) if not already done
What NOT to do:
– Do not perform abdominal thrusts (Heimlich maneuver) on infants—this can cause internal injury
– Do not blindly sweep finger into baby’s mouth—this can push the object deeper
– Do not interfere if baby is coughing forcefully—coughing is effective
Part 4: Nursing Strikes (Breast Refusal)
What Is a Nursing Strike?
A nursing strike is when a baby who has been breastfeeding well suddenly refuses to breastfeed. This can be distressing, but it is usually temporary and not a sign that baby is ready to wean .
Common Causes of Nursing Strikes
Research identifies several factors contributing to breast refusal :
| Factor | Percentage |
|---|---|
| Playfulness and distraction | 50.0% |
| Recent vaccination (within 12 days) | 48.6% |
| Mother’s education level | 67.1% |
| Recent acute stress in mother | 41.4% |
| Perceived inadequate milk production | 35.7% |
Additional factors: Use of a pacifier, changes in breastfeeding routine, illness (ear infection, teething), changes in breast milk taste (due to hormones, medications, or diet), or strong maternal stress response.
What to Do During a Nursing Strike
1. Stay calm: Stress can affect milk production and baby’s willingness to feed.
2. Increase skin-to-skin contact: Hold baby against bare chest to encourage natural feeding instincts.
3. Offer breast when baby is sleepy or calm: Babies may feed better when drowsy.
4. Try different positions: Walking while feeding, side-lying, or laid-back positions.
5. Minimize distractions: Feed in a quiet, darkened room.
6. Maintain milk supply: Express or pump regularly to protect supply and avoid engorgement.
7. Check for illness: Look for signs of ear infection, thrush, or teething.
8. Be patient: Most nursing strikes resolve within a few days to a week.
When to seek help: Contact your health visitor or lactation consultant if the strike persists beyond a few days, baby shows signs of illness, or you’re concerned about hydration or weight gain.
Part 5: Weaning from Breastfeeding
When to Consider Weaning
Weaning is the process of gradually replacing breast milk with other foods and drinks. The World Health Organization recommends exclusive breastfeeding for the first 6 months, followed by continued breastfeeding alongside appropriate complementary foods for up to 2 years or beyond .
Reasons for weaning may include:
– Infant-led weaning: Baby naturally loses interest in breastfeeding (usually after 12 months)
– Mother-led weaning: Personal choice, returning to work, or medical reasons
– Natural progression: As baby eats more solids, breastfeeding gradually decreases
How to Wean Gradually
The golden rule: Gradual is better for both of you.** Slow weaning allows baby’s nutritional intake to adjust gradually and helps your milk supply decrease without causing engorgement or mastitis.
Step-by-step approach:
1. Replace one feeding at a time: Start by dropping the least preferred breastfeed (often the midday feed) and replace with expressed milk in a cup (if under 12 months) or whole cow’s milk and solids (if over 12 months).
2. Wait several days: Allow your body and baby to adjust before dropping another feed.
3. Drop feeds slowly: Continue replacing one feed every few days to weeks, depending on baby’s age and your comfort.
4. Offer comfort in other ways: Provide extra cuddles, attention, and soothing alternatives as breastfeeding sessions decrease.
For babies under 1 year: Breast milk or formula must remain the primary source of nutrition. Replace dropped breastfeeds with expressed breast milk or formula in a cup. Cow’s milk is not recommended as a main drink before 12 months.
For babies over 1 year: Dropped breastfeeds can be replaced with whole cow’s milk (300-400 ml daily) offered in a cup, plus a balanced diet of solids.
Managing Engorgement During Weaning
When you reduce breastfeeding, your breasts may become uncomfortably full. This is normal as your body adjusts production .
Do’s:
– *Gradual weaning: This is the most effective way to prevent severe engorgement .
– Express to comfort: If breasts feel painfully full, hand express or pump just enough to relieve pressure—not to empty completely . This signals your body to reduce production without triggering more milk.
– Cold packs: Apply cold compresses or ice packs wrapped in a cloth after expressing to reduce swelling and discomfort .
– Pain relief: Take recommended doses of paracetamol or ibuprofen as needed .
– Cabbage leaves: Clean, refrigerated cabbage leaves placed inside your bra can provide comfort. Use only until swelling subsides, as prolonged use may decrease milk supply too much .
– Gentle movement: Very gently moving breasts with palms of hands in a warm shower may help .
– Rest: Get as much rest as possible during this transition .
Don’ts:
– Don’t bind breasts tightly: This can lead to blocked ducts or mastitis.
– Don’t stop expressing completely if engorged: Complete cessation with severe engorgement can increase inflammation risk .
– Don’t ignore severe pain or redness: These could indicate mastitis requiring medical attention.
What Doesn’t Help with Engorgement
A 2020 Cochrane review found that many commonly recommended interventions lack evidence of effectiveness, including :
– Cabbage leaves (though still used for comfort, evidence limited)
– Breast compresses
– Acupuncture
– Gua sha or other massage
– Therapeutic ultrasound
– Enzyme therapy
Signs You May Need Medical Help During Weaning
Contact your GP or midwife if you experience:
– Red, hot, swollen area on breast
– Fever or flu-like symptoms (possible mastitis)
– Severe pain not relieved by simple measures
– Hard lump that doesn’t resolve with gentle expression
Summary: Key Points at a Glance
| Topic | Key Messages |
|---|---|
| Hunger cues | Feed at early cues (rooting, sucking fists). Crying is late hunger cue . |
| Fullness cues | Baby releases breast, slows sucking, appears content, turns away . |
| Burping | Try three positions; gentle patting; burp mid-feed and end; not all babies need burping. |
| Choking | Mild: let baby cough, turn to side. Severe: 5 back blows + 5 chest thrusts (AHA 2025) . |
| Nursing strike | Common causes: distraction, vaccination, maternal stress. Stay calm, skin-to-skin, offer when sleepy . |
| Weaning | Gradual is best. Drop one feed at a time, wait days between changes. |
| Engorgement during weaning | Express to comfort, cold packs, pain relief, rest. Avoid abrupt cessation . |
**Key Resources:**
– Association of Breastfeeding Mothers: www.abm.me.uk
– La Leche League: www.laleche.org.uk
– National Breastfeeding Helpline: 0300 100 0212
– NHS Start for Life: www.nhs.uk/start-for-life
*References available upon request. Key sources: WHO ,扬州市妇女儿童医院 , Jalali F et al. J Med Life 2021 ,深圳市儿童医院 (AHA 2025 guidelines) , NDC Institute , HealthyChildren.org (AAP) .*
a.本站所有文章,如无特殊说明或标注,均为本站原创发布。
b.任何个人或组织,在未征得本站同意时,禁止复制、盗用、采集、发布本站内容到任何网站、书籍等各类媒体平台。
c.如若本站内容侵犯了原著者的合法权益,可联系我们进行处理。









暂无评论内容